You run a control, the analyser flashes a code like 1-3s or 2-2s, and now you have a decision to make with a patient waiting. Reject the run and repeat? Bin the reagent? Recalibrate? Or was that flag nothing to worry about? For staff running near-patient testing without a laboratory-science background, the Westgard rules can read like an alphabet soup that turns a 30-second quality check into a guessing game. Worse, the most common mistake costs you time and money: discarding a perfectly good run because a single control drifted slightly past a warning line.
Here are the Westgard rules explained in plain terms: each rule reduced to one sentence and the single action it should trigger. You also get a decision table that links every rule to the kind of error behind it and its most likely cause, and a clear line between a warning and a rejection so you stop repeating runs you never needed to repeat.
First, what your QC is actually telling you
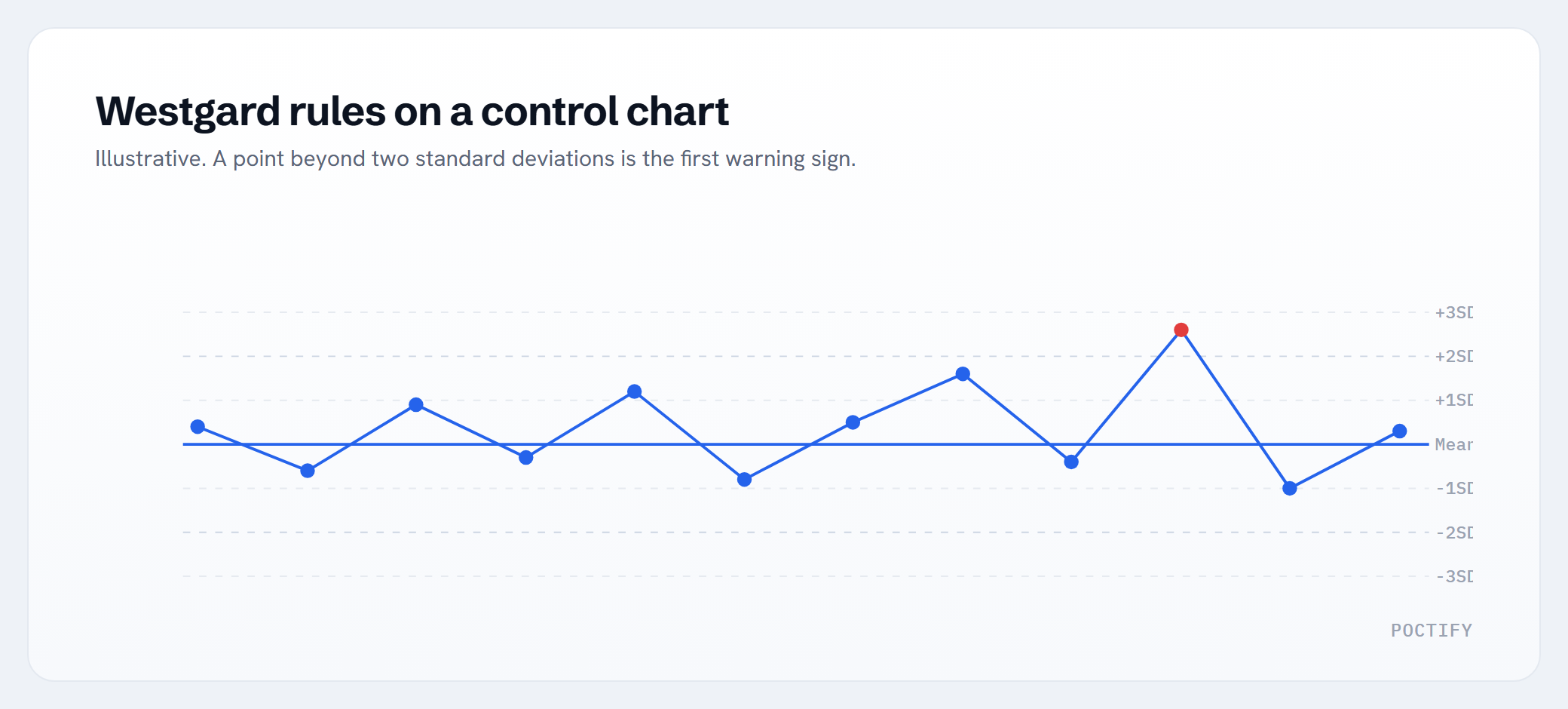
Quality control (QC) means running a sample with a known, stable value before or alongside patient samples. Each control has a target (the mean) and an expected spread (the standard deviation, or SD). Most analysers plot results on a chart with lines at 1, 2 and 3 SD above and below the mean. The Westgard rules are simply a set of patterns on that chart that flag when a result, or a string of results, is unlikely to be down to normal variation.
The whole point of a multirule approach is to catch real problems while raising as few false alarms as possible. Used well, it tells you two things: whether something has gone wrong, and what kind of wrong it is.
Random error versus systematic error
Every rule points to one of two failure types, and the distinction drives your next step.
- Random error is scatter. Results jump around unpredictably: one high, one low, with no consistent direction. Think bubbles, a poorly mixed control, a one-off pipetting slip, or electronic noise.
- Systematic error is a shift. Results drift to one side of the mean and stay there. Think a new reagent lot, a calibration that has moved, or an instrument slowly going out of tune (drift).
Random error tends to fix itself on a clean repeat. Systematic error does not: repeat all you like, the bias stays until you address the cause.
The Westgard rules explained, one sentence each
Here is the classic multirule set in plain terms, with the single action each should prompt.
1-2s: the warning, not a verdict
One control result falls just beyond 2 SD from the mean. This is a warning only. It happens by chance roughly 1 run in 20 even when everything is fine, so the action is to look, not to reject: check the other rules below before you do anything. This is the single most misread flag in point-of-care testing.
1-3s
One control result falls beyond 3 SD from the mean. Reject the run and investigate. A result this far out is rarely chance, and it usually points to random error such as a bubble, a wrong or short sample, or a one-off handling slip.
2-2s
Two results in a row land beyond the same 2 SD limit on the same side (two consecutive controls high, or two consecutive controls low). Reject the run. This is a textbook systematic error: a recent calibration, a fresh reagent lot or developing drift has shifted your method.
R-4s
Within the same run, one control sits above +2 SD and another sits below -2 SD, so the spread between them tops 4 SD. Reject the run. This is random error: imprecision from bubbles, poor mixing, a clot, or an unstable instrument.
4-1s
Four consecutive results all fall on the same side of the mean, each beyond 1 SD. Reject the run (some labs treat this as a strong warning on a single control). This is systematic error, typically early calibration drift or a reagent ageing toward the end of its life.
10x
Ten results in a row fall on the same side of the mean, even if each one is small. Reject the run. A run of ten one-sided points is not coincidence: it is a quiet, steady bias from drift, a calibration shift, a reagent lot change or a temperature problem.
Decision table: read the flag, find the cause, take the action
| Rule | Plain meaning | Error type | Most likely cause | Action | |——|—————|———–|——————-|——–| | 1-2s | One result past 2 SD | Neither yet | Normal chance variation | Warning only. Inspect, do not reject. Check the other rules | | 1-3s | One result past 3 SD | Random | Bubble, wrong/short sample, one-off slip | Reject, repeat the control | | 2-2s | Two in a row past 2 SD, same side | Systematic | New reagent lot, calibration shift | Reject. Recalibrate or check the lot before patients | | R-4s | One control +2 SD, another -2 SD in a run | Random | Imprecision, mixing, clot, unstable instrument | Reject. Remix, degas, check the analyser | | 4-1s | Four in a row past 1 SD, same side | Systematic | Calibration drift, ageing reagent | Reject. Recalibrate, check reagent expiry/storage | | 10x | Ten in a row, same side of mean | Systematic | Drift, calibration, lot change, temperature | Reject. Recalibrate, review reagent lot and storage |
A useful habit: when a run is rejected, name the error type out loud before you act. If you say “random”, a clean repeat with fresh control material is often enough. If you say “systematic”, repeating is a waste of time. Go to the calibration, the reagent lot or the instrument.
Stop binning good runs: warning versus rejection
The costliest confusion in routine QC is treating a 1-2s warning as a rejection. On a single level of control, a 1-2s flag will appear by chance about 5% of the time. If you reject and repeat every one of those, you throw away good results, burn reagent, and train the team to distrust the analyser.
The discipline is simple. A 1-2s is a prompt to glance at the rest of the picture. Only escalate to a rejection if a true rejection rule (1-3s, 2-2s, R-4s, 4-1s or 10x) also fires. If none does, the run is good. Release it.
The flip side matters just as much. A string of results that never crosses 2 SD but sits stubbornly on one side (the 4-1s and 10x patterns) is easy to wave through because no single point looks alarming. Those are the quiet systematic shifts that put biased patient results into circulation. Trusting your eyes alone, you will catch the dramatic 1-3s and miss the slow drift.
Let the log do the maths
Applying six rules across multiple control levels, run after run, by eye is where the system breaks down on a busy clinic floor. People are good at spotting a single point past 3 SD and poor at counting ten consecutive points on one side of a mean while a patient waits.
This is exactly what a digital QC log is for. Record each control result and the software evaluates the full multirule set automatically across every level, then flags only the runs that genuinely warrant action. It separates the warning from the rejection for you, keeps the Levey-Jennings chart up to date, and holds a timestamped, auditable record for inspection. The result is fewer false rejections, no missed drift, and a QC routine that does not depend on whoever is on shift remembering what 4-1s means. Many quality standards, including ISO 15189:2022 for medical laboratories, expect documented QC with retrievable records, so consult the published standard for the exact wording that applies to you. If you want the underlying chart logic, our piece on reading Levey-Jennings charts pairs naturally with this one, and you can see worked examples per test in the Analyte Explorer.
This article is for educational and operational guidance only. It is not medical advice and does not replace your laboratory’s standard operating procedures or your device manufacturer’s instructions for use.
Talk to POCTIFY
If your team is unsure when a QC flag means stop and when it means carry on, that uncertainty is fixable. POCTIFY builds digital point-of-care testing tools tailored to each clinic, including QC logging that applies the Westgard rules for you and surfaces only the runs that matter, and that works with the devices and systems you already use. If you would like a calmer, clearer QC routine, talk to POCTIFY about what would suit your setup.
Frequently asked questions
Should I reject a run when I get a 1-2s flag?
No. A 1-2s flag is a warning only. One control result just past 2 standard deviations happens by chance roughly 1 run in 20 even when everything is working. Inspect the run and check the other Westgard rules. Only reject if a true rejection rule (1-3s, 2-2s, R-4s, 4-1s or 10x) also fires. Otherwise the run is good and you can release it.
What is the difference between random and systematic error in QC?
Random error is unpredictable scatter: results jump high and low with no consistent direction, usually from bubbles, poor mixing or a one-off slip. Systematic error is a one-sided shift that stays put, usually from a new reagent lot, a calibration change or instrument drift. The 1-3s and R-4s rules point to random error; the 2-2s, 4-1s and 10x rules point to systematic error.
Do I have to use all six Westgard rules?
Not always. The full multirule set gives the best balance of catching real problems while limiting false alarms, but some tests with very stable performance use a simpler single rule such as 1-3s. The right combination depends on how critical the test is and how your method performs. Follow your QC plan and your device manufacturer’s guidance, and document which rules you apply.
A control failed. What should I do first?
Identify the error type before you act. If the flag points to random error (1-3s or R-4s), a clean repeat with fresh, well-mixed control material is often enough. If it points to systematic error (2-2s, 4-1s or 10x), repeating will not help: check the calibration, the reagent lot and its storage, and the instrument. Do not release patient results from a rejected run until the cause is resolved.
Can software apply Westgard rules automatically?
Yes. A digital QC log records each control result and evaluates the full multirule set across every control level automatically. It separates warnings from rejections, keeps the chart current, flags only the runs that need attention, and holds a timestamped record for audit. This removes the manual counting that is easy to get wrong on a busy clinic floor.